
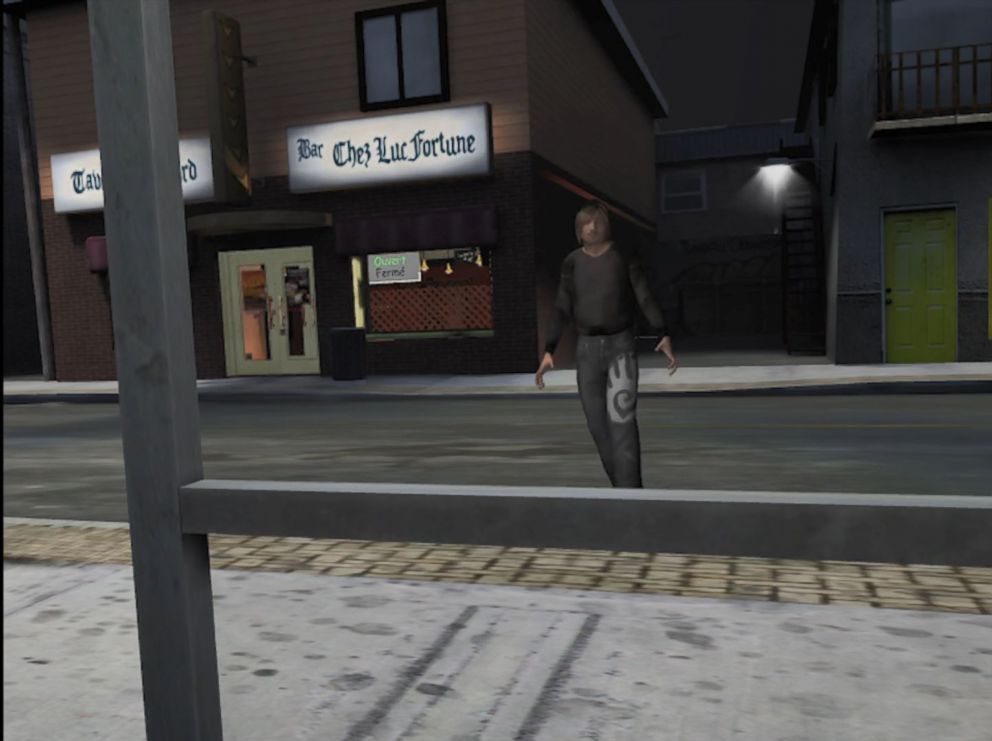
You’re leaving a bar at night and a man follows you out to an isolated bus stop. You try to ignore him but he won’t back off, pressing in closer and closer.
You can choose to rip off your goggles and be transported back to your therapist’s office.
Or you can stay in the hyper-realistic virtual environment, created by psychologists to help survivors of sexual assault and rape face their trauma and find healing.
“For rape victims, the idea is that in therapy we need to help people confront their fears, and one way is that we have to go places where we don’t go normally,” Dr. Stéphane Bouchard, a clinical psychologist and professor at the University of Quebec in Outaouais, told ABC News.
Bouchard is spearheading a team of researchers that are using virtual reality (VR) technology to help sexual assault victims address their darkest experiences effectively and safely.

"We need to help people confront their fears."
With VR technology, researchers can recreate the environment of a bar, a dark alley or even an actual rape scene to help patients “practice ways to get out of this and not panic,” Bouchard said.

“We can go very far in the rape scene, where you are actually being raped,” Bouchard continued. “The idea is that we can go to these personal moments in therapy where people don’t really want to get in touch with.
“As a therapist, we need to touch on that. VR allows us to progressively go on that.”

Using VR technology as a tool to treat anxiety disorders and post-traumatic stress disorder (PTSD) has gained momentum in the medical community over the last 20 years.
VR exposure therapy -- the method of slowly exposing a patient to their main source of anxiety -- has proven useful for treating war veterans who suffer from PTSD.
While re-exposing victims of sexual assault to a rape scene may raise some eyebrows, exposure therapy as a concept -- even with the absence of virtual reality technology -- is a commonly used treatment method for victims of sexual trauma.
Dr. Mindy Mechanic, a professor of psychology at California State University, Fullerton, who specializes in trauma, told ABC News that the two most commonly used therapy methods for treating PTSD in sexual assault victims are prolonged exposure therapy and cognitive processing therapy.
“Essentially both of those approaches are aimed at helping an individual break through their avoidance of trauma,” Mechanic said. “Traumatic events by definition are very overwhelming in terms of emotions.
“Getting in touch with them can bring back those feelings of being out of control, so consequently people avoid thinking about them, avoid talking about them,” she added. Resultantly, Mechanic said, “the emotions never get fully processed.”
“One of the core principles” for both cognitive processing therapy and prolonged exposure therapy for victims of sexual trauma, according to Mechanic, is that “emotions need to be fully experienced and processed in order to fully get rid of the PTSD symptoms.”
“As part of therapy, people have to re-experience and re-live the traumatic event many, many times over and over again, in a guided situation until the strength of their emotions is extinguished,” she said.
In traditional therapy, the exposure is done by having a patient write out a narrative of the account multiple times, and working through it with their therapist over the course of multiple sessions.
“Initially, sexual assault survivors will give you their narrative in the past tense, after they’ve done it a number of times, and they are starting to feel more comfortable, you get them to narrate in the present tense,” she added.
“At the beginning, the trauma controls them, and then at the end of therapy you want the person to control the narrative, so that they are no longer overwhelmed by memories,” she said.
“You need to get their anxiety up enough so that it will then extinguish, if you don’t get their anxiety up enough then it’s not helpful,” Mechanic said. “It has to be up enough so that it will be able to come down.”
Bouchard told ABC News that the exposure therapy using VR employed by him and his team of researchers at the University of Quebec in Outaouais’ Cyberpsychology Lab is only done when a patient is “ready to do that.”
Bouchard emphasized that “exposure with or without VR is part of a whole therapy process” and is “not just one thing we do” but is “part of something larger.”
“It’s part of a therapy where it is trying to face their fear,” Bouchard said. “For PTSD, it would mean going to places you avoid going to.
“In virtual reality, we do exactly the same thing, we go to bars and dark alleys and bus stations in the goggles, in a safe environment and we go back to these rape scenes,” he added.
Bouchard said the overall response from rape victims who have tried the VR exposure therapy has been “very positive.”
“People were a bit worried that it would go too fast, but they realized that it would really go at their own pace,” he said. “It allows them to stay in control when we do the exposure, which is something very hard to control otherwise.”
Bouchard, who has been researching in the intersection of virtual reality and clinical psychology since 1999, said its popularity among mental health professionals and patients has skyrocketed in recent years.
“The big problem we had 10 years ago was the cost of the hardware and the software,” he said, adding that as technology has improved, VR headsets have become more widely accessible and much cheaper.
The virtual reality environments developed by Bouchard and his team are currently only available to mental health professionals. Patients who are interested in using it can seek to access it through their mental health care provider.
Dr. Albert “Skip” Rizzo, the director of medical virtual reality at the University of Southern California’s Institute for Creative Technologies, told ABC News that he and his team of researchers had been using VR exposure therapy to treat military veterans with PTSD for years when they were confronted with “the crisis of sexual trauma in the military.”
In 2014, they started working on a VR therapy program specifically aimed at helping victims of sexual assault in the military.
“We just completed our initial safety and feasibility trial,” he said, adding that they hope to present their findings to the medical community in May.
“This is emotionally evocative content,” he said. “Whenever you develop these things you want to run small trials so you make sure you are not going to hurt anyone.
“We are very happy that No. 1, we didn’t hurt anyone, and No. 2, we got good data,” he said of their research.
During his more than 20 years of research in VR exposure therapy, Rizzo said some common questions he has been asked are “Why would you do that to someone? Why would you make them go back?”
Rizzo said those who say “you are going to re-traumatize people” are often “not that well-trained in scientific literature.”
“Prolonged exposure, along with cognitive processing therapy, are considered and endorsed by the APA [American Psychological Association] as evidence-based treatments,” he said. “It’s hard medicine for a hard problem, no doubt.”
He emphasized, however, that VR exposure therapy aimed at helping people overcome trauma is in no way meant to be easy.
“It is painful, it is hard, you are peeling back the scab on the wound,” he said. “But you see patients start to feel empowered, start to feel stronger and the anxiety starts to extinguish through repeated exposure.”
“This is a very hard therapy that requires a well-trained clinician,” he said. “If people are not well-trained, then you can run into problems.”
As a result, they are “very strict” about who gets access to the software, Rizzo said.
“I know it sounds scary,” he added of VR exposure therapy, “but again, it comes down to bad therapy, whether it’s in VR or any other way, poses a risk.”
Rizzo said while there could always be “cases that we don’t hear about,” in his research, “the fears that people have about re-traumatizing patients have not been documented.”
Of the negative reactions he has seen from patients, Rizzo said the “worst of it” is “motion sickness.”
“We are not saying this is the magic bullet, but we are trying to see who can benefit from this treatment,” he said. “Perhaps the digital generation.”
“There is a place for the traditional imaginal exposure,” he added, “but there is also a place for VR.”
While there is a lot of hype and excitement about VR in the medical community now, Rizzo said it “has been around for a long time.”
“I have been doing research on it since 1996; the technology really sucked way back then,” he said. “But the technology has now caught up with the vision.
“Now that the technology has gotten better, VR really stands poised to make a difference,” he added. “It’s not a magic bullet, but for the areas where it’s well-matched, and exposure therapy is one of those areas, I think we can really make a real difference.”



