
Dr. Mary Bassett addressed an audience in Boston last October.
"This epidemic is complicated, and like all epidemics, it tracks along fissures in our society,” Bassett, a professor at Harvard's public health school, told the crowd.
Bassett was talking about the opioid crisis, but her turn of phrase was prescient.
She just as easily could have been referring to the COVID-19 epidemic, for which the United States has emerged as the epicenter, making up a third of the world's infections and a quarter of its deaths by May. Like past epidemics, COVID-19 is exposing cracks that already existed in our health system -- and widening them.
"Any time you have a whole population exposed to a disease, it reflects the structural underpinnings and the failures of our society," Bassett told ABC News in April.

The United States has the largest gross domestic product in the world and one of the highest per capita. But its health doesn't reflect that wealth. Instead, Americans are sicker than residents of other high-income countries. The United States leads the developed world in diabetes prevalence, and has a higher heart disease death burden than other high-income countries, data show. Asthma rates in the U.S. rise every year. And all three chronic conditions are considered comorbidities that raise patients' risk for developing severe and deadly COVID-19 complications.
Our chronically ill populace comprises one layer of America's strained health system. Stark inequality that's concentrated in communities of color makes up another. Then there's the health care system itself, experts tell ABC News. Despite spending twice as much on health care as other high-income countries, studies show the U.S. fails to produce healthier citizens. Instead, the sick sometimes face crushing medical debt and the uninsured cycle through our emergency rooms.
Without a nationalized public health response system in place, experts say government leaders in many cases panic and throw money at acute problems like COVID-19, but show little appetite for proactive investments to bolster population health.
Working in tandem, those failings appear to have worsened the United States' COVID-19 outbreak, experts said. Decision-makers can use that list of failings as a roadmap to make improvements now, experts added, or they can once again neglect the cracks in the system, until the next pandemic hits.
While the United States is among the world's wealthiest countries, there are stark differences in how that wealth is concentrated.
According to the Brookings Institution, the net worth of a typical white family is $171,000, nearly 10 times greater than a black family's typical net worth of $17,150.
That wealth gap trickles down into various opportunity gaps, which are reflected in disparities in infection and death rates during the coronavirus pandemic, as well as a black-white health gap that existed before COVID-19.
Preliminary demographic data released by the Centers for Disease Control and Prevention (CDC) appears to bear this out. Thirty-three percent of hospitalized COVID-19 patients are black, compared to 18% of residents in the surrounding community, suggesting an overrepresentation of black Americans among hospitalized patients, the agency notes. In New York City, the country's biggest COVID-19 hotspot, more than 20,000 residents have died, black and Latino residents are more likely to die of COVID-19 than their white and Asian neighbors.
SLIDESHOW: Coronavirus outbreak sparks global health emergencyThose disparities include direct health care access problems, including higher uninsured rates among Latino and black Americans than among white Americans.

There are also less obvious health disparities than access to doctors or health insurance. A lifetime of social conditions, including where Americans are born, live and play, shape their health. So do education and employment opportunities. Housing plays a role. Incarceration and immigration status matter, experts say.
As COVID-19 has devastated the black community, it's also unmasked the effects of structural racism to the wider public, according to Dr. Camara Jones, an epidemiologist and past president of the nonprofit American Public Health Association, who has also worked for the CDC.
"COVID-19 was rolled out as an equal opportunity infector, and all of a sudden, the black bodies are piling up so quickly that people cannot normalize it or ignore it," Jones said.
Black Americans fare worse than white Americans on nearly every measurable metric of health, including cancer death, HIV infection and maternal mortality rates.
MORE: Coronavirus map: Tracking the spread in the US and around the worldCOVID-19 has made those disease disparities strikingly clear. Because black Americans are more likely to have diabetes, obesity and asthma, the underlying health problems that predispose them to develop severe COVID-19 complications, they're also more likely to be hospitalized or die from the new disease.
"This is not genetic," Bassett stressed. "This is related to the way in which we structured our society."
While there's some variation between individuals when it comes to fitness, genetics and luck, "the reasons we get sick, or not, have more to do with our society than any biological features that we may have as individuals," Bassett said.

An analysis published last month by New York University's Furman Center, for example, found that the strongest neighborhood factors linked to high COVID-19 rates were having a large share of black and Hispanic residents; having a high proportion of overcrowded apartments and having a large share of residents without college degrees.
MORE: Front-line COVID doctor: We want student loan forgiveness, not hazard paySince college-educated workers are more likely to be able to work remotely than people without a college education, people without degrees risk being exposed to the disease on the job, or are forced to choose between their health and a paycheck in some cases. And because fewer than 1 in 5 black workers and 1 in 6 Hispanic workers are able to work remotely, according to the Economic Policy Institute, on-the-job exposure disproportionately affects people of color.
"What it is showing is that we have huge schisms of opportunity and experience and exposure in a society structured by race," Jones said. "We actually have a system that does that. We have a system of opportunity and assigning value in this country, and that’s what we call racism," she added.
"If we were not to react to this data, we would be doing what racism often does — especially structural racism — showing itself through inaction in the face of need," Jones said.
While improving health care, education and neighborhood safety are important, those problems won't be solved overnight.
President Donald Trump addressed the disproportionate number of black Americans dying from COVID-19 during a White House press conference in April. "This is a real problem, and it's showing up very strongly in our data," he said, adding that his administration would do everything in its power to support African Americans and address COVID-19 racial disparities.
In the short-term, Jones and Bassett pointed to the importance of addressing black Americans' acute needs during the outbreak. Frontline workers, and not just doctors and nurses, but also subway employees, bus drivers, janitors and delivery people, need personal protective equipment and paid sick leave.
MORE: In NYC, 'stark contrast' in COVID-19 infection rates based on education and race"The important thing here is to make it easier for people to avoid exposure, just like it’s important to make it easier for people to eat healthy food," Bassett said.
In Bassett's mind, that includes challenging the impulse to blame those who fall ill for getting infected.
"All that anyone who gets infected will have been guilty of is breathing," she said.
The U.S. spends more on health care than any other country, with little to show for it.
Even before the pandemic, health insurance costs for middle-class families were rising, to say nothing of the 27.5 million Americans who were uninsured pre-pandemic. Many Americans are perpetually on the edge of falling into medical debt, with 1 in 3 people reporting that they wouldn't be able to cover an unexpected $400 medical bill without borrowing money or selling their belongings.
With no national health care system and 33 million Americans filing for unemployment in recent weeks, citizens' access to affordable health care is only likely to get worse.
"Of course that will have a bearing on health insurance, because so many of us have our health insurance through our jobs," Bassett said.
The interdependent relationship between health and housing creates a relentless cycle, according to Leo Beletsky, a professor of law and health sciences at Northeastern University.
Medical debt and ill health are risk factors for being homeless, he explained. "When you lose housing, you’re more susceptible to a lot of health issues. People who have health issues are more likely to lose housing," Beletsky said. Without reliable and affordable health services, the homeless lean heavily on the hospital system.
"Most folks who are homeless can’t access primary care outside of the emergency room, and they utilize the ER far more than is really necessary. Their care bills end up being extremely large without really conferring much benefit to those folks," Beletsky said.
"We basically help when it's too late. It costs a lot of money, requires heroic interventions and people continue being sick," he added.
"It's very much a microcosm for our health care system in general. Rather than investing in prevention, we dump an enormous amount of resources at a time when it really is too late."

There's also significant overlap between being incarcerated and being homeless, another vulnerable group that's been hard hit by COVID-19. According to a report by the Prison Policy Initiative, formerly incarcerated people are nearly 10 times more likely to be homeless than the general population. In New York City, half of people who are released from prison move directly into the city's shelter system.
"It's one situation of mass living to another situation of mass living," said Dr. Alysse Wurcel, an infectious disease physician at Tufts Medical Center.
Shelters, jails and prisons contain a population of sicker-than-average people living in tight quarters, where social distancing is impossible and sanitation is often an afterthought. It's an environment ripe for disease spread.
Shelters in Seattle, Boston and San Francisco have all reported COVID-19 outbreaks.
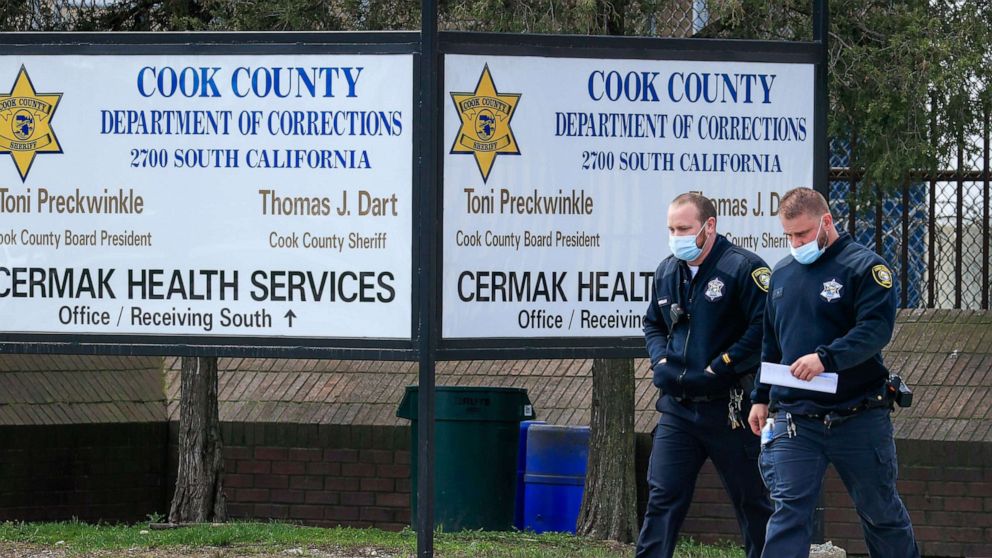
Jails and prisons have fared even worse. Chicago's Cook County jail emerged as one of the nation's COVID-19 hotspots after more than 800 detainees and correctional officers tested positive. More than 14,500 people in prison have tested positive for COVID-19 since the start of the outbreak, according to the Marshall Project, which is tracking prison data from all 50 states and from the Federal Bureau of Prisons.
Instead of flattening the curve, the number of new infections is doubling each week. More than 5,000 corrections officers have tested positive for the disease, an ABC News analysis found.
"I wish there were more attention paid to the fact that incarceration is a comorbidity factor," said Kate Chatfield, senior adviser for legislation and policy at The Justice Collaborative, a criminal justice research and advocacy organization.
The prison population is also disproportionately black and poor. According to the Federal Bureau of Prisons, nearly 40% of the prison population is black, compared to 13 percent of the overall population.
"All of the things that would lead to bad health outcomes," Chatfield added. "And that's just upon custody."
Being in detention presents its own health risks. Every year served in prison reduces life expectancy by two years, an analysis published in the American Journal of Public Health found.

The COVID-19 infection numbers being released by prisons and jails are likely an undercount, experts say. It's unclear how many jails and prisons are thoroughly testing their populations, if they're testing at all.
"If you’re not finding cases, you're an ostrich in the sand," said Wurcel, who is consulting Massachusetts jails on how to respond to COVID-19. "We are learning that rapidly in Massachusetts. It’s pretty much everywhere."
One of the many eye-opening moments of the pandemic was watching U.S. governors bid against one another for ventilators, during a time when it was believed that there would be a severe ventilator crisis.
Although that anticipated shortage did not come to pass, residents in states with governors who could negotiate well would live, it seemed, while others would die.
Lack of national coordination has deepened division between states, resulting in some states adopting strict lockdown measures, while others have opened back up for business. It's also fueled a brutal cultural war between those who say their livelihood depends on returning to work and those who fear dying from the virus, should it be allowed to spread unchecked.
The splintered response to the pandemic in the U.S. has not only pitted Americans against one another, but also appears to be part of a larger trend of not preparing for the future, experts say.
Between 2008 and 2017, for example, funding cuts resulted in 55,000 jobs cut from local health departments across the country. Dozens of rural hospitals have closed over the past decade. And in 2018, President Donald Trump disbanded the global health security and biodefense unit, which is responsible for pandemic preparedness.
"Our job was to be the smoke alarm," Beth Cameron, the first director of the unit, wrote in the Washington Post. "Keeping watch to get ahead of emergencies, sounding a warning at the earliest sign of fire — all with the goal of avoiding a six-alarm blaze."
"You are doing something to prevent harm so you never see that harm realized," Beletsky said. Prevention is a hard sell, he added. It's far easier for politicians to justify spending money on a crisis that's already in motion, like COVID-19.
"There you can justify pretty unlimited resources."
"People can’t wrap their heads around working upstream and preventing problems," according to Beletsky. In turn, lack of upstream investment in affordable housing and health care, in preventative medicine and paid sick leave, in education and safe and healthy neighborhoods, have all exacerbated the United States' COVID-19 crisis, experts said.
Whether the harsh light COVID-19 has shone on outbreaks in prisons and shelters, and on racial disparities in COVID-19 deaths will force policymakers to invest in communities of color and in public health preparedness or usher in criminal justice reform, remains to be seen.
"There's a lot of talk about getting back to normal after COVID-19, but there's a range of issues where getting back to normal isn't desirable," Beletsky said.
"There are rays of hope in that. There are also a lot of reasons to be pessimistic."
Tune into ABC at 1 p.m. ET and ABC News Live at 4 p.m. ET every weekday for special coverage of the novel coronavirus with the full ABC News team, including the latest news, context and analysis.


